Some of you will say “not more Wenckebach. He is obsessed with the topic”. Actually, that is correct as ECGs with Wenckebach block seem to come to life.
Although I have done it many times, let us review the typical Wenckebach AV block.
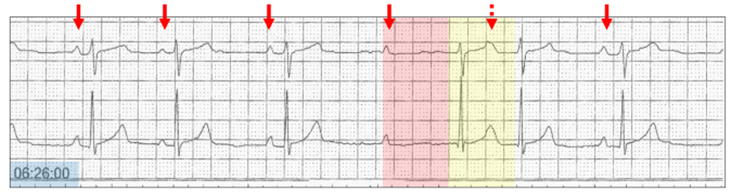
- Progressive prolongation of the PR interval (red highlight)l culminating in a non-conducted P wave (red arrow).
- AV node rests and conduction returns (yellow highlight).
There are a number of other typical features, but not relevant to this discussion.
Because there are so many variations of Wenckebach AV block, I will also add another definition, which is very helpful in diagnosis.
This is the absolute Wenckebach AV block, because if you see these three features, then you are correct in diagnosing Wenckebach AV block.
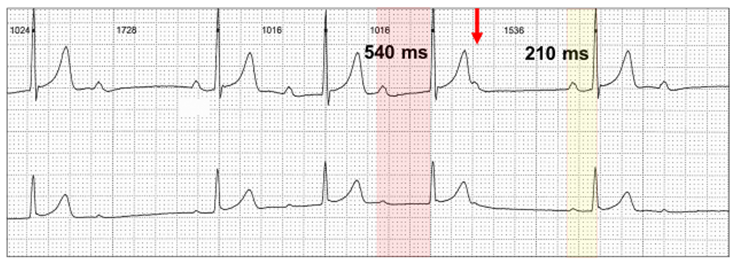
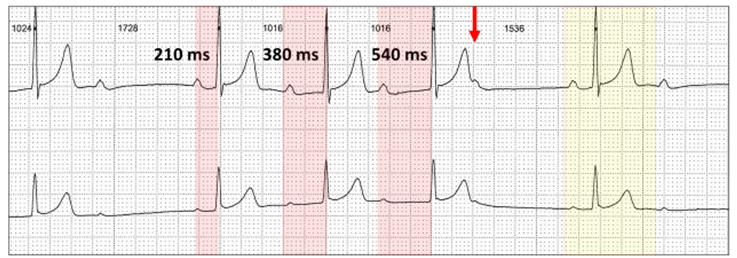
- The PR interval is longest immediately before the dropped beat (red highlight).
- There is a non-premature, non-conducted P wave (red arrow)
- The PR interval is shortest immediately after the dropped beat (yellow highlight).
Even though I call these absolute footprints, there are occasions when these features are not present, and the ECG appearances appear unusual. Because they differ from the typical, I will refer to them as atypical Wenckebach AV block.
Let us look at examples of atypical Wenckebach AV block.
Most occur overnight with the nocturnal times in blue highlight.
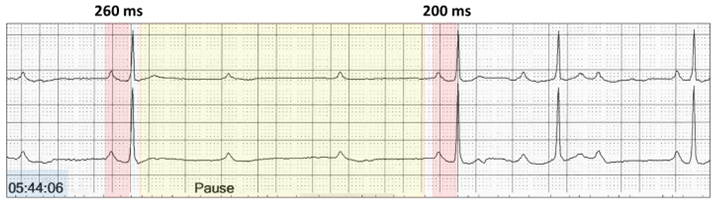
There is more than one blocked beat, and the P-P intervals lengthen during the pause. This is a feature of many of the Wenckebach ECGs and is a parasympathetic phenomenon which is physiologic, and I refer to broadly as vagal hypertonia, although many would reserve the term for severe and symptomatic cases.
Another bizarre ECG:
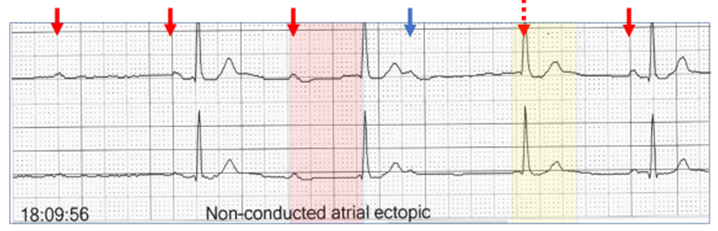
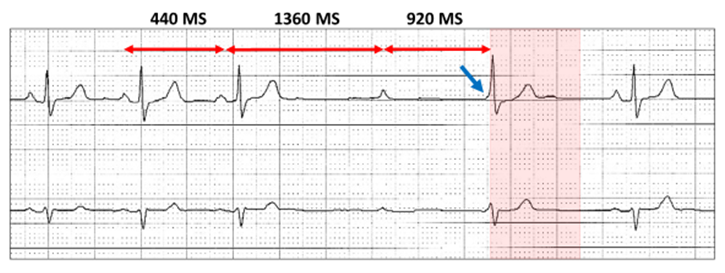
There is a dramatic increase in the PR interval after the first beat in the sequence (red highlight) without sinus slowing (arrows). The next P wave (blue arrow) is conducted after a very long PR interval or is a junctional escape beat (yellow highlight). The next P wave (red stippled arrow) is concealed within the QRS and does not conduct. The annotation states that there is a non-conducted atrial ectopic (blue arrow), although the timing confirms it is sinus.
Another example of a marked increase in the PR interval with a bizarre appearance.
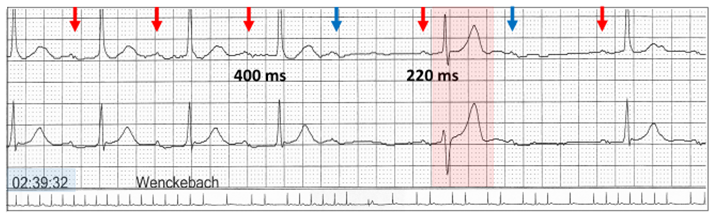
Sinus rhythm (red arrows) with Wenckebach AV block, but is there a dropped beat? There is a very long PR interval (red highlight) or maybe a junctional escape beat (yellow highlight). The next P wave (red stippled arrow) is concealed within the T wave and conducts with PR prolongation as AV conduction is partially refractory.
Sometimes, it is obvious that a junctional escape beats terminates a Wenckebach sequence.
There is both sinus slowing and Wenckebach AV block. Because of sinus slowing, there is a junctional escape beat (red highlight) and the next sinus P wave occurs at the commencement of the QRS (blue arrow).
It is possible for an escape beat to fuse with a sinus beat.
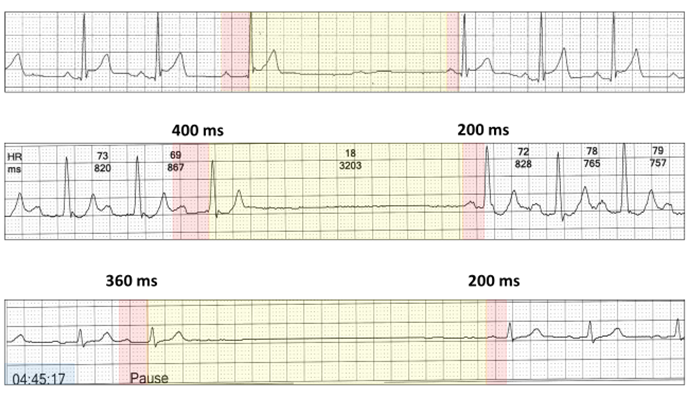
This one could have a number of alternatives. There is nocturnal Wenckebach AV block with dropped beats (blue arrows). Following the first pause, the PR interval shortens to 220 ms, but now the QRS is different (red highlight) to the sinus complexes. The upstroke of the QRS is identical to the sinus beats, suggesting that this is a fusion beat with maybe a fascicular escape beat.
With nocturnal vagal hypertonia, the sinus bradycardia may be profound (red highlight) and can be an isolated nocturnal event (yellow highlight):

Even sinus arrest (yellow highlight) may interrupt Wenckebach sequences (yellow highlight):
Once again, it’s all in the timing.
Harry Mond