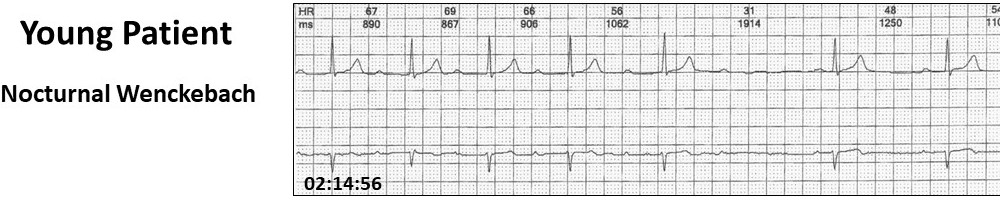
This Holter monitor tracing in a 44-year old male caused a lot of excitement at Cardioscan this week. There were about 12 bradycardia episodes overnight.
The report simply said “Wenckebach AV block”. Clinically, rather than visually, this may be correct, nevertheless, it does not fulfil the footprints of Wenckebach summarised below.
Footprints
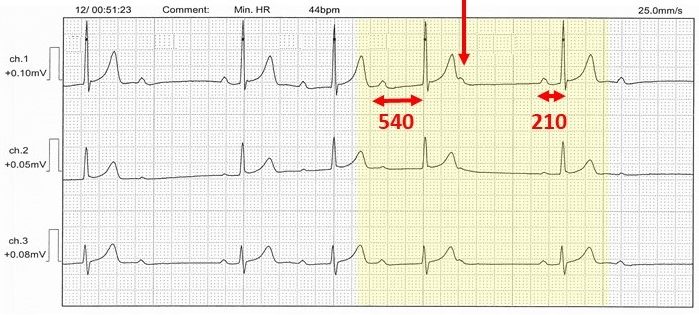
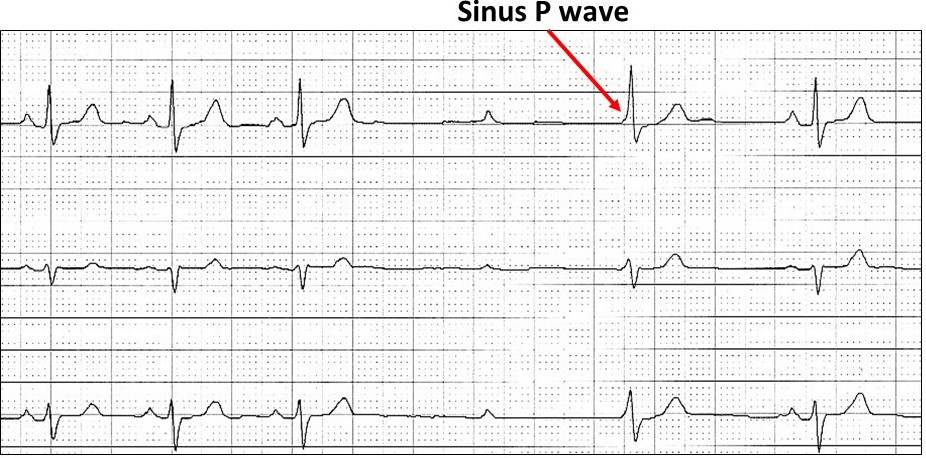
- Non-conducted sinus P wave (vertical arrow)
- The PR interval is longest immediately before the dropped beat
- The PR interval is shortest immediately after the dropped beat
In our case study, there were one or two dropped beats and the PR sequences don’t fit.
Clinically, there are two types of Wenckebach AV block:
The Wenckebach is generally AV nodal, nocturnal, innocent, asymptomatic and related to vagal tone. The incidence on Holter monitoring is 4-6% and reversed with atropine and exercise. Rare intra-Hisian Wenckebach AV block is worse with atropine.

This usually occurs with conduction tissue disease and may progress onto higher degrees of AV block. If in the young, think of congenital AV block.
Let us return to the case study!
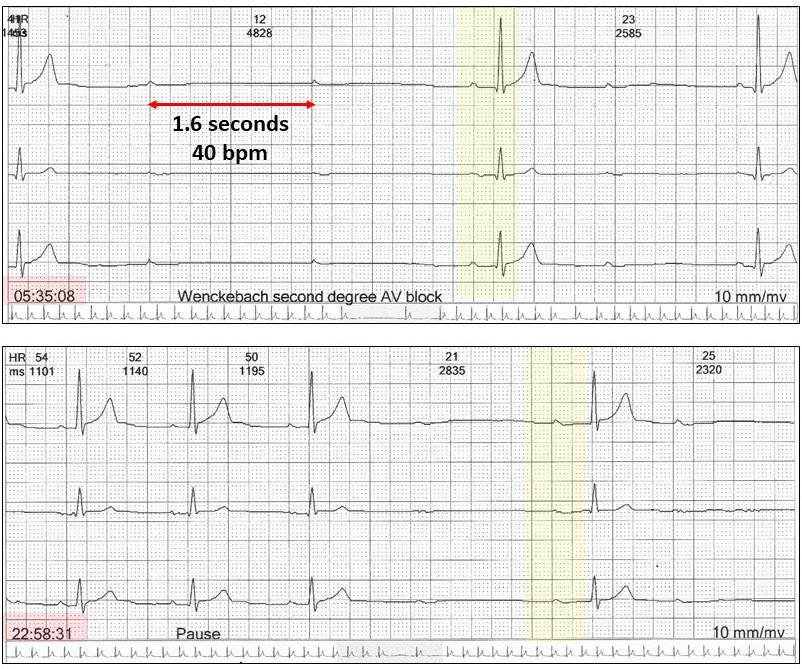
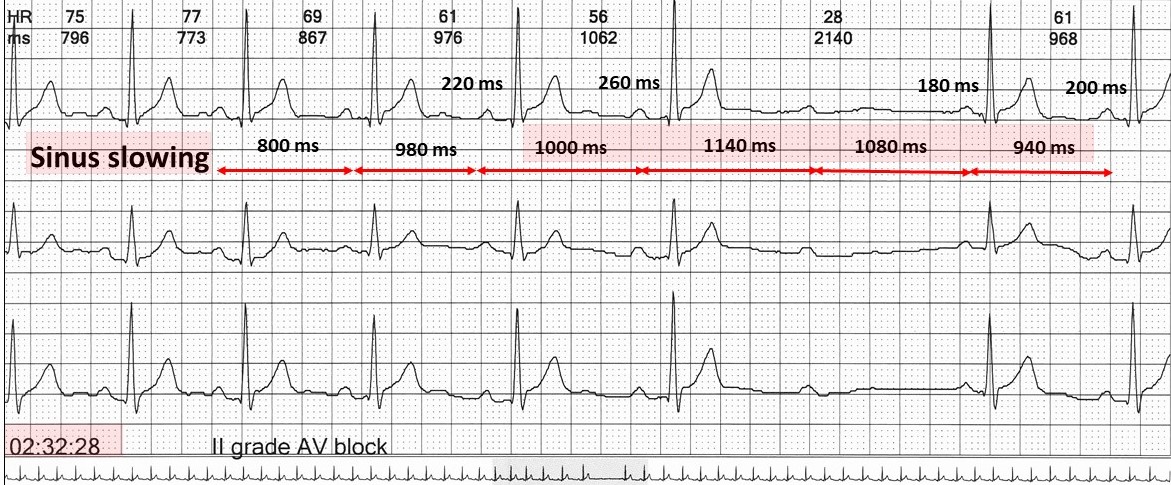
There is at least second-degree AV block and the PR intervals after the dropped beats are variable and longer than before. It is most likely these P waves do not conduct and the subsequent QRS complexes are junctional escape beats. If this is Wenckebach, then it is very atypical, but 85% of all Wenckebach sequences are atypical anyway. I call this “atypical- atypical Wenckebach AV block” meaning it is Wenckebach but doesn’t look like it!!
The presence of a junctional escape beat is also very common with nocturnal Wenckebach.
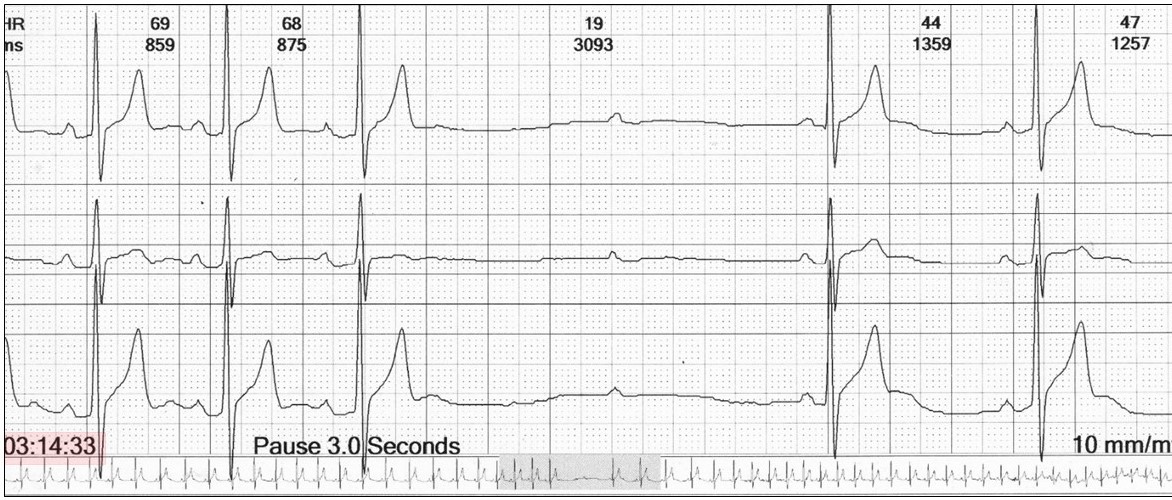
The case study showed a number of significant pauses overnight.
The 24-hour Holter rate histogram showed bradycardia, but no other abnormalities.
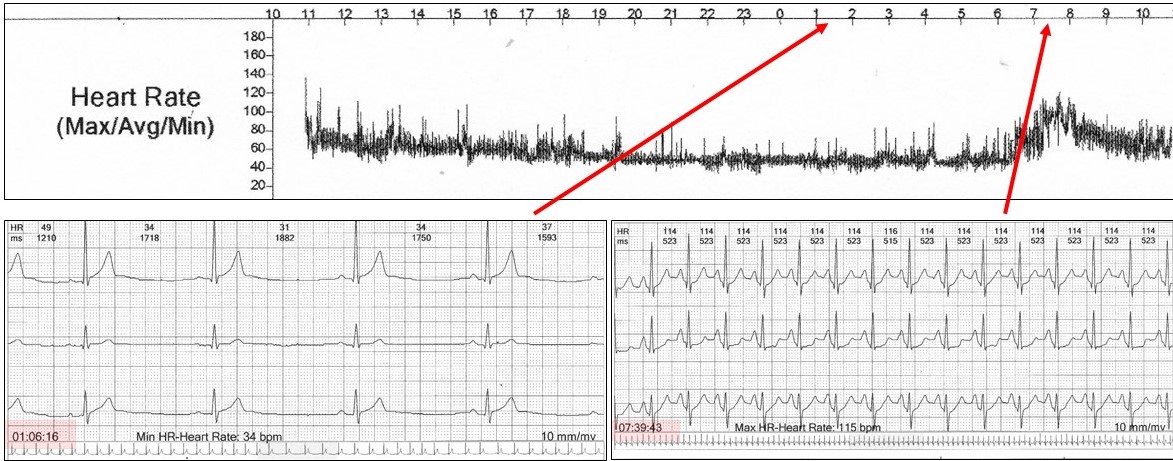
The other feature in this case study was sinus bradycardia, rate 40 bpm during the AV block.
Wenckebach AV block in the young, is commonly associated with nocturnal sinus rate slowing.
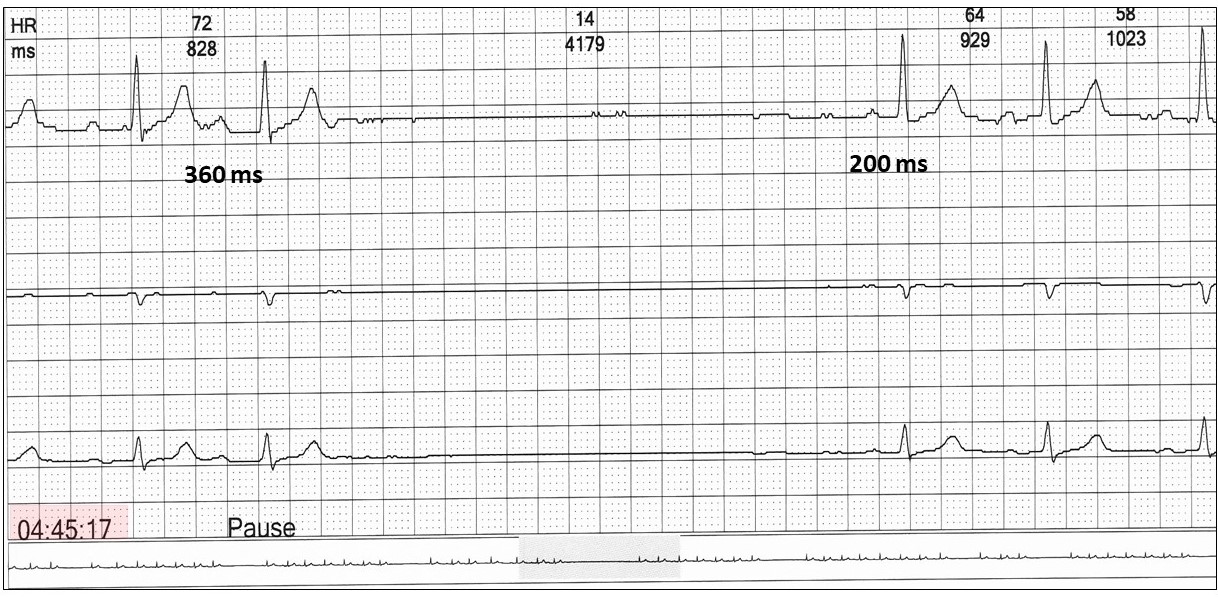
Sometimes it can be extreme!
And even associated with asystole (27-year old female with frequent episodes overnight)!
So, what are we dealing with in this case study!
There are asymptomatic episodes of sinus bradycardia and second-degree AV block as a result of vagal hypertonia. Simply put, but not always electrophysiologically correct, the right vagus nerve innovates the sinus node and the left the AV node. It is normal to have nocturnal sinus slowing and maybe first-degree AV block. With an exaggerated vagal response in the young, this may deteriorate further and with vagal hypertonia, we see the responses as shown.
Provided the patient is asymptomatic, nothing more need be done. If symptomatic, then interventional therapy may be required. In the past, dual chamber pacing was required. Today cardioneuroablation is being offered in some centres. This involves the electrophysiological ablation of the vagal ganglia, which innervate the sinus and AV nodes in the superior vena cava, right atrium and left atrium.
Results are preliminary and permanent pacing may be required. Remember, if you are unsure about Wenckebach, then call it second degree AV block.
Harry Mond