As we saw in our last session, not all bundle branch blocks are boring.
What do you think of this ECG?
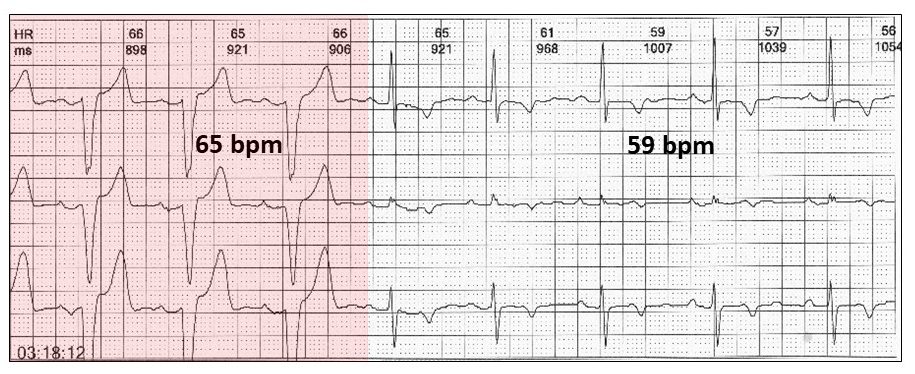
There are sinus P waves and identical PR intervals prior to each QRS; narrow and bundle branch block. As the sinus rate slows, the bundle branch block (red highlight) disappears. This is a rate dependent or more correctly a tachycardia dependent bundle branch block.
Here is another more subtle example.

Note that the diagnosis would have been missed, if only the top ECG was available.
The clues lie in the P waves and PR intervals before each QRS. It is frequently mistaken for an idioventricular rhythm:

There are no P waves and obviously no PR intervals before wide QRS complexes (red highlight). What is also important are the fusion beats (yellow highlight) confirming two foci; one sinus and the other ventricular.
Rate dependent bundle branch blocks may be present, even when the rhythm appears to be a “permanent” bundle branch block.

A premature ventricular ectopic with a compensatory pause (red highlight) results in a single sinus beat with a narrow QRS (yellow highlight).
Another frequent misdiagnosis with tachycardia dependent bundle branch blocks is ventricular tachycardia:
 During the Holter tracing, there was obvious rate dependent bundle branch block (above) with rates above 60 bpm. With exercise and sinus tachycardia (below), the appearance was that of ventricular tachycardia, but in an asymptomatic patient. There was a clue with an atrial ectopic and a short compensatory pause, releasing a sinus P wave (red highlight).
During the Holter tracing, there was obvious rate dependent bundle branch block (above) with rates above 60 bpm. With exercise and sinus tachycardia (below), the appearance was that of ventricular tachycardia, but in an asymptomatic patient. There was a clue with an atrial ectopic and a short compensatory pause, releasing a sinus P wave (red highlight).
Is there a bradycardia dependent bundle branch block?
It is said to be rare. It is if you don’t look for it!!

There is a sinus pause and the next sinus beat has a bundle branch block.
The widening of the QRS with a bradycardia is usually quite subtle.

I usually like to finish with something that is rarely commented on.
This ECG shows a “borderline” right bundle branch block. In some leads, the QRS is actually 0.16 sec.

Is there anything else to report on?
When I was a young cardiologist, we didn’t have echocardiography and depended on other ways to diagnose atrial septal defects. This included the 12-lead ECG with a right branch block. (We also used stethoscopes in those days).
There is, however, an ECG sign that I was unaware of in those days, that may catch the eye of the reporter, particularly in patients with migraine or a suspected paradoxical cerebral embolus.
It is called the crochetage sign; a hook (red highlight) like a crochet needle.

Features:
- Subtle notch in the QRS of inferior leads
- In association with a RBBB, then high incidence of ostium secundum ASD (or even a patent foramen ovale – think of embolic CVA)
- Higher incidence with larger defects
- May disappear after closure
Remember, it’s all in the timing
Harry Mond